
Optimizing Surgical Port Access for Improved Visualization and Closure
- sutureease
- Mar 31
- 4 min read
In laparoscopic and robotic surgery, surgical port access is the gateway to everything that follows: exposure, dissection, suturing, and specimen management. Yet port strategy is often treated as setup work rather than a core part of surgical performance.
For modern teams, optimizing surgical port access is a two-part goal: maximum visualization during the procedure and a consistent, secure fascial closure at the finish. This is where technique, instrumentation, and standard work intersect, especially as programs take on more complex patients and higher case volumes.
The Strategic Importance of Surgical Port Access During Port Placement
“Triangulation” is an efficiency lever. When ports are placed without a clear access plan, the downstream effects are predictable:
Instrument clashing that reduces range of motion and forces constant repositioning
Compromised visualization that obscures critical anatomy and increases the chance of unintended tissue contact
Ergonomic strain as surgeons work at awkward angles for the duration of the case
Robotic-assisted surgery increases the stakes. Once ports are docked, small placement choices can become big workflow constraints. And every port carries a second responsibility: a fascial defect that must be managed appropriately at the end of the case.

Visualization Doesn’t End When the Case Is “Done”
One of the highest-risk transitions in minimally invasive surgery is the move from operative work to exit. Specifically, closure performed without clear visualization of what’s happening below the abdominal wall.
Traditional manual closure methods can introduce uncertainty when teams are working with limited exposure or challenging depth. A closure approach that supports visualization (direct or indirect via laparoscope) helps teams confirm what matters:
The needle captures a robust fascial bite (not superficial tissue)
No bowel or omentum is inadvertently incorporated into the closure line
The needle path avoids unintended internal contact and reduces avoidable bleeding risk
The point isn’t to add gadgets. It’s to remove guesswork at the moment where the case transitions from “surgical success” to “recovery trajectory.”
The Surgical Port Access Lifecycle: Entry to Secure Exit
A useful way to build consistency is to treat surgical port access as a lifecycle, not a single action. You’re setting up a safe, controlled exit.
Standardizing the “Safe Exit” for ≥10 MM Ports
Across the clinical literature, trocar site hernias (TSH) remain a recognized source of morbidity, with reported incidence ranges that are not trivial. Many teams standardize closure for ports 10 mm or larger because these sites carry higher risk compared to smaller ports.
High-BMI patients add a practical complication: increased distance from skin to fascia makes both access and closure more difficult. That is exactly where “good enough” closure can become inconsistent across surgeons, shifts, and service lines.
What Changes When You Standardize With a Dedicated Closure Workflow?
When teams standardize exit steps, they’re usually trying to achieve three things:
Repeatable fascial capture across patient body types
A closure sequence that can be performed under vision when needed
A predictable number of steps so closure doesn’t become the variable part of the case
How Crossbow™ and Longbow™ Support a Tool-Based Approach to Surgical Port Access Closure
Suture Ease approaches closure as part of the port access lifecycle and offers a full line of fascial closure solutions intended to match different clinical demands.
Crossbow™ for Standard Port Access Closure
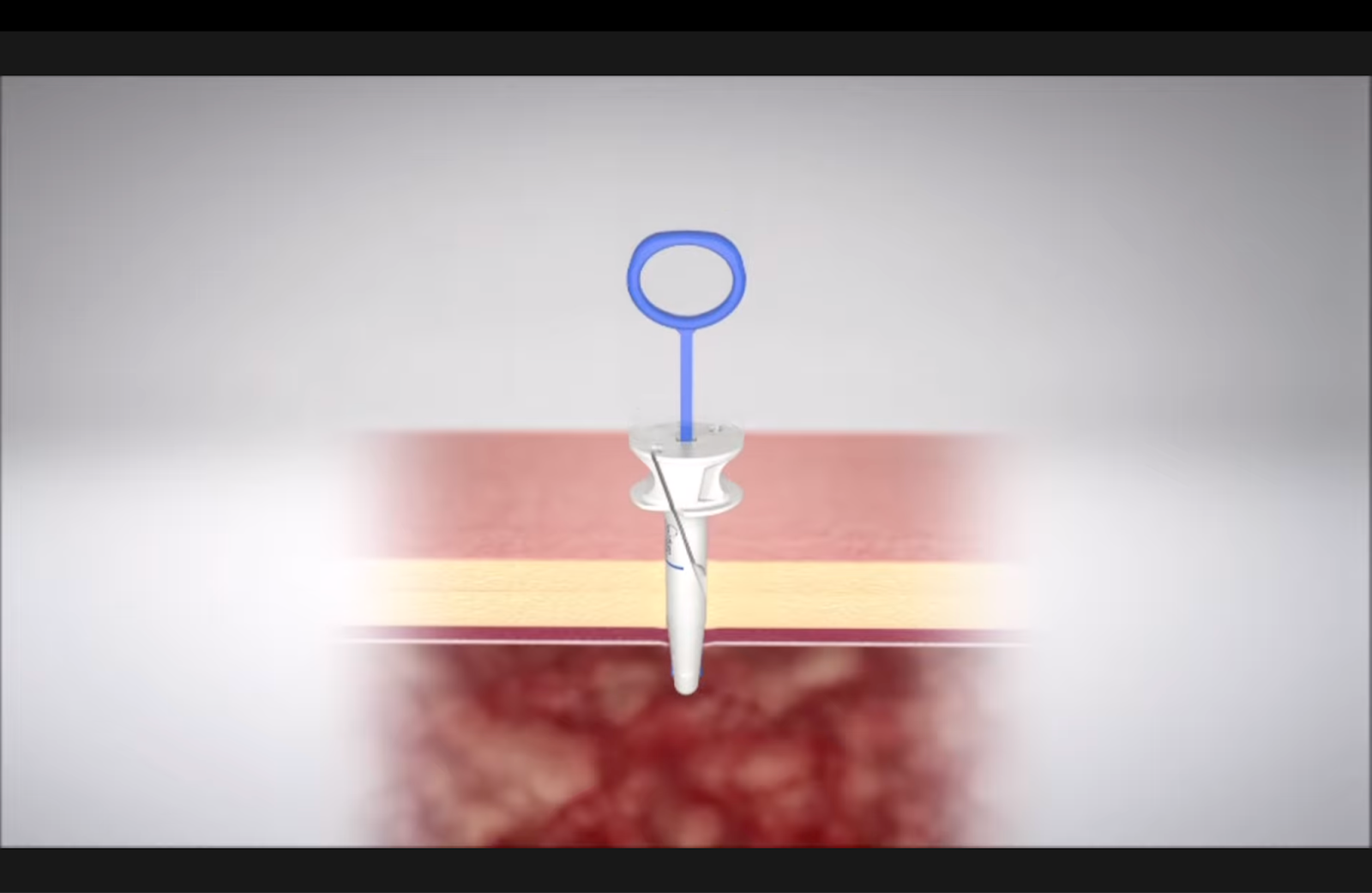
CrossBow is designed around a guided workflow with a snare-loop concept that supports consistent capture and suture retrieval without “fishing” for suture ends. Practically, that means fewer improvised maneuvers at the end of the case and a closure step that is easier to teach and repeat.
Phase of Surgical Port AccessCommon Failure ModeWhat “Optimized” Looks LikePort planning / triangulationClashing, poor angles, unstable visualizationPorts placed to support reach, camera view, and ergonomicsIntra-op instrument exchangeExtra time from awkward approach pathsClear lanes for instruments; fewer forced repositionsEnd-of-case closure decisionInconsistent closure at ≥10 mm portsStandard criteria for which ports get fascial closureClosure executionBlind passes, shallow capture, extra attemptsTool-based closure option that supports controlled capture and under-vision confirmation when needed
Longbow™ for Deep Port Sites in High-BMI Cases
LongBow is an extended-reach option intended for deeper abdominal walls, where angle, depth, and visualization challenges can make standard closure workflows less predictable. The goal is straightforward: maintain controlled handling and consistent fascial closure even when tissue depth increases.
Adjustable Bite Strategy When Tissue Quality Varies
Tissue quality is not uniform. A closure workflow that supports selecting an appropriate fascial bite, rather than forcing a single bite size in every situation, helps teams balance closure integrity with patient-specific considerations. This is particularly relevant when tissue is fragile or at higher risk of suture pull-through.
A Practical Framework for Teams: Port Access Planning and Closure Execution
Here’s a simple way to align surgeons and perioperative teams around surgical port access consistency.
Phase of Surgical Port Access | Common Failure Mode | What “Optimized” Looks Like |
|---|---|---|
Port planning / triangulation | Clashing, poor angles, unstable visualization | Ports placed to support reach, camera view, and ergonomics |
Intra-op instrument exchange | Extra time from awkward approach paths | Clear lanes for instruments; fewer forced repositions |
End-of-case closure decision | Inconsistent closure at ≥10 mm ports | Standard criteria for which ports get fascial closure |
Closure execution | Blind passes, shallow capture, extra attempts | Tool-based closure option that supports controlled capture and under-vision confirmation when needed |
Quick Checklist: Building a Consistent “Safe Exit”
Standardize which ports require fascial closure (commonly ≥10 mm) and document it in service-line preference cards
Use a closure method that supports controlled capture, especially in high-BMI patients and deep port sites
Encourage under-vision confirmation when closure conditions are uncertain (depth, limited exposure, difficult angle)
Value-Based Care: Why Materials and Admin Staff Should Care
From a hospital perspective, optimizing surgical port access is a cost and consistency decision. A single trocar site hernia can lead to readmission, additional imaging, potential reoperation, and patient dissatisfaction. When closure steps vary by operator or tool availability, the system absorbs that variability later.
A portfolio approach matters because one device rarely fits every scenario. Standardizing access and closure across General Surgery, GYN, and Urology is easier when teams have the right tool for standard cases and for deep or difficult port sites.
Get a Better Way to Manage Surgical Port Access With Suture Ease
Optimizing surgical port access means treating port placement and closure as one continuous responsibility. Better triangulation supports better visualization. Better visualization supports safer closure. And standardized, tool-based closure reduces variability at the moment that matters most: the exit.
Contact us for more information about CrossBow™ and LongBow™ and how they can support your surgical port access closure workflow.



Comments